

Introduction
Functional Neurological Disorder (FND) is a condition at the intersection of neurology and psychiatry, where patients experience neurological symptoms such as weakness, tremors, non-epileptic seizures, or gait disturbances, without an identifiable structural lesion. Historically misunderstood and often stigmatized, FND was once framed as a diagnosis of exclusion or as a purely psychogenic condition. However, in recent years, neuroscience has begun to illuminate its underlying mechanisms, revealing a complex interplay of functional brain networks that govern motor control, sensory processing, emotion regulation, interoception, and the sense of agency.
This article aims to unpack the current understanding of the brain areas involved in FND using a network-based approach. We will bridge the gap between academic knowledge and clinical relevance, providing insights valuable to both professionals and educated members of the public.
A Visual Overview of the Brain in FND
To help illustrate this emerging perspective, the following diagram outlines the key brain regions implicated in FND and their associated functions:
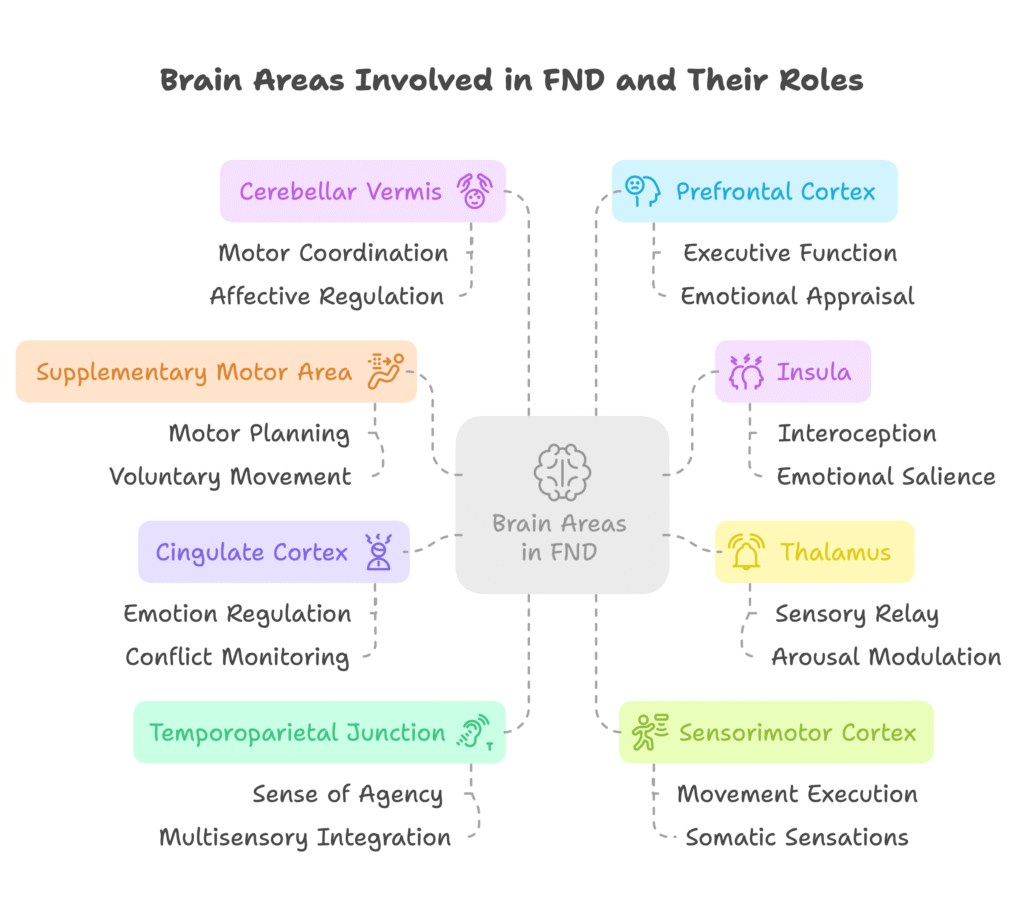
Each region plays a unique role in motor, sensory, emotional, and integrative processes that are often disrupted in patients with FND. These dysfunctions are not the result of damage but of altered connectivity, network efficiency, and maladaptive responses to stimuli or stressors.
1. Prefrontal Cortex: Executive Control and Emotional Appraisal
The prefrontal cortex (PFC) is central to executive functions—decision-making, attention, working memory—and is also deeply involved in emotional regulation and cognitive reappraisal. In FND, studies suggest reduced top-down control from the PFC over subcortical regions like the amygdala and basal ganglia, leading to impaired regulation of emotional stimuli.
Functional MRI (fMRI) studies have shown hypoactivation of the dorsolateral PFC during tasks that require executive function in FND patients, along with altered responses to emotional cues. This may contribute to the emergence of symptoms during emotional or interpersonal stress.
Clinical relevance: Difficulty modulating emotional responses can trigger or perpetuate symptoms like non-epileptic attacks or sudden motor dysfunction.
2. Supplementary Motor Area (SMA): Planning and Initiating Movement
The SMA is involved in the initiation and planning of voluntary movements. It is closely connected with the motor cortex and basal ganglia. In FND, patients often experience motor symptoms without corresponding activation of the SMA, suggesting a disruption in the voluntary motor command pathway.
Additionally, the SMA shows abnormal connectivity with limbic areas, indicating a potential role in emotion-triggered motor dysfunction. This may help explain how emotional triggers can lead to paralysis, tremors, or gait disturbances.
Clinical relevance: Motor symptoms may not reflect a lack of effort or “faking,” but rather an abnormal disconnection between intention and execution.
3. Insula: Interoception and Emotional Salience
The insular cortex serves as a hub for interoception (the sense of internal bodily states) and integrates emotional, sensory, and cognitive signals. It determines the “salience” or significance of stimuli.
In FND, the insula may be hyperresponsive or misinterpret benign bodily sensations as threatening, contributing to symptom perception. fMRI studies have shown increased activity in the anterior insula during symptom provocation in patients.
Clinical relevance: Patients often report intense, unexplained bodily sensations that precede or accompany FND episodes, underscoring the insula’s role.
4. Cingulate Cortex: Emotion Regulation and Conflict Monitoring
The anterior cingulate cortex (ACC) is essential for emotional regulation, error detection, and conflict monitoring. It acts as a bridge between the emotional limbic system and the cognitive executive system.
In FND, altered ACC function may contribute to poor integration of emotional and cognitive information, leading to exaggerated bodily responses or reduced awareness of bodily control.
Clinical relevance: The cingulate may be involved in the internal experience of “something being wrong” without a clear external cause, reinforcing symptom persistence.
5. Thalamus: Sensory Relay and Arousal Modulation
The thalamus is a major relay center for sensory and motor signals and is key to regulating consciousness and alertness. In FND, altered thalamic connectivity has been observed, especially in patients with sensory symptoms or dissociative seizures.
Disrupted communication between the thalamus and cortical areas may lead to impaired sensory processing or dissociation during stress.
Clinical relevance: FND symptoms like numbness or dissociative seizures may stem from thalamic dysregulation.
6. Sensorimotor Cortex: Execution and Sensation
While not damaged in FND, the sensorimotor cortex often shows altered patterns of activation, especially during movement attempts. Studies show hypoactivation during voluntary movement and abnormal activation during involuntary movements or functional tremors.
This supports the concept of impaired motor execution, not due to structural lesions, but to functional disconnection.
Clinical relevance: Neurological examinations may appear inconsistent not because the patient is malingering, but because of altered functional activation.
7. Temporoparietal Junction (TPJ): Sense of Agency and Multisensory Integration
The TPJ is involved in integrating sensory information and generating a sense of agency—the feeling that “I am the one causing this movement.”
In FND, TPJ dysfunction may contribute to the feeling that movements or sensations are happening “to” the patient, rather than being self-generated. This aligns with experiences of dissociation and loss of control.
Clinical relevance: Loss of agency is a core component in many FND presentations and is crucial in diagnosis.
8. Cerebellar Vermis: Motor Coordination and Affective Regulation
The cerebellum, and particularly the vermis, is increasingly recognized for its role in emotional regulation alongside motor coordination. Its connections with the limbic system suggest a pathway through which affective states influence motor function.
Studies show increased cerebellar activation in patients during motor symptom provocation, indicating its potential role in FND motor control.
Clinical relevance: Gait disturbances and postural instability in FND may be linked to cerebellar involvement, especially under emotional stress.
FND as a Network Disorder: Beyond Local Lesions
One of the most important insights from modern neuroscience is that FND is not due to a problem in one specific brain area. Instead, it reflects disruptions in large-scale brain networks:
- The default mode network (DMN)
- The salience network
- The sensorimotor network
- The central executive network
Disruptions in the balance and connectivity of these networks underlie the varied symptoms of FND. For example, increased activity in the salience network may explain heightened symptom focus, while underactivation in the motor network explains voluntary movement difficulties.
Implications for Treatment and Recovery
Understanding FND as a disorder of network dysfunction opens the door to more targeted interventions:
- Psychological therapies (CBT, psychodynamic therapy) to retrain interpretation of interoceptive signals
- Physiotherapy to restore motor pathways and voluntary control
- Education to reduce stigma and validate the experience
- Neuromodulation and mindfulness to improve network regulation
Clinicians can use this neurobiological model to explain symptoms in a validating, non-judgmental way, improving engagement and outcomes.
Conclusion
FND is not a mystery or a “wastebasket” diagnosis. It is a complex condition grounded in the real dysfunction of how the brain processes, integrates, and responds to information. The affected brain areas are part of dynamic, interacting networks that explain the wide range of symptoms patients experience.
By recognizing and respecting these mechanisms, we can better support patients, educate the public, and dismantle the stigma that has long surrounded functional disorders. Bridging neuroscience with clinical care is the key to understanding what happens beyond the symptoms—and ultimately, beyond the impact.